
Introduction:
The goal of breast augmentation surgery, commonly referred to as augmentation mammoplasty, is to improve the size and form of the breasts by cosmetic surgery. This treatment has a long history that dates back to the late 1800s, and it has changed dramatically over time to rank among the most common cosmetic surgeries performed globally.


History of breast augmentation surgery:
Historical Methods of Breast Augmentation in the 1800s
Historical documents from the 1800s show that there was not much information available on particular breast augmentation treatments. But there were also anecdotal reports and infrequent attempts at breast augmentation around this time, frequently involving risky and unusual techniques. These approaches were principally grounded in experimental procedures, cultural practices, and anecdotal evidence.
Compared to modern surgical techniques, breast augmentation treatments were significantly less sophisticated in the 1800s. Attempts to increase breast size and shape at this time were frequently motivated by experimental techniques, cultural customs, and anecdotal evidence. Although specific breast augmentation operations in the 1800s are not well documented, historical records indicate that a number of hazardous and unusual methods were used. An overview of the items in use at that time is shown below:
Injections of paraffin:
Occasionally, injections of paraffin wax were utilized in an effort to augment breast volume. Using this technique, melted paraffin wax was injected straight into the breasts. On the other hand, a number of side effects were linked to paraffin injections, such as tissue stiffening, granuloma formation, infection, and migration of paraffin droplets.

Various Substances Injected:
The purpose of injecting different drugs into the breasts was to increase their size and form. These materials included ground rubber, glass balls, ivory, and even the cartilage of oxen. Nevertheless, issues like tissue necrosis, allergic responses, migration, and infection were common with these materials.
Transfers of Fat:
Autologous fat grafting, also name for fat transfers, is the process of taking fat tissue from other body parts—like the thighs or abdomen—and injecting it into the breasts to give them more fullness. But in the 1800s, fat transfers were carried out in unsterile conditions and without the use of current procedures, which led to high rates of infection, necrosis, and fat absorption.
Tissue Exchanges:
On rare occasions, attempts were made to enlarge the breasts using tissue transplants from other regions of the body. In order to boost volume, donor sites had to have tissue, such as fat or muscle, transplanted into the breasts. However, there were a number of serious hazards related to tissue transplantation, such as tissue rejection, donor site morbidity, and unsatisfactory cosmetic results.
Utilizing External Electronic Devices:
In the 1800s, women frequently turned to wearing accessories or devices that were intended to make their breasts appear larger. These apparatuses included padded bras, corsets, and mechanical breast-lifting and shaping devices. Although these devices could improve breast look in the short term, they did not offer long-term augmentation and over time frequently resulted in pain and physical abnormalities.
Not to mention a dearth of regular operating procedures and safety measures, the 1800s were marked by a lack of medical expertise and anatomical comprehension. Consequently, a great deal of the breast augmentation techniques employed at this time were risky, experimental, and frequently had unfavorable side effects. The 20th century saw the development of safe implant materials and contemporary surgical procedures, which made breast augmentation surgery a feasible and widely accepted operation.
A cosmetic surgical treatment called breast augmentation surgery, or augmentation mammoplasty, aims to improve the size and form of the breasts. With a lengthy history that dates back to the late 19th century, this operation has undergone tremendous evolution to rank among the most popular cosmetic surgeries performed globally.
Silicone Injections and implements:
The use of silicone injections for breast augmentation gained popularity in the 1940s and 1950s. Nevertheless, there were significant health hazards connected to these injections, such as the development of granulomas and the migration of silicone to other body regions.
Saline Implants and Contemporary Approaches;
During the 1960s and 1970s saline filled implants started replacing silicone implants because of safety issues. Saline implants were seen as an option, in case of rupture as the body could safely absorb the saline solution. In the following decades from the 1980s to the 1990s progress, in methods and implant technology continued to enhance the safety and success rate of breast augmentation procedures.
Regulatory Concerns and Contemporary Safety Standards:
In the early 1990s, US silicone implant use was put on hold due to safety concerns. However, silicone implants were restored to the market in 2006, subject to stringent controls and oversight by regulatory authorities, following considerable research and safety reviews.
Trends of the Present and the Future:
Remarkably, one of the most popular cosmetic surgeries done globally even today is breast augmentation surgery. Better outcomes that seem more natural have been achieved by improvements in surgical methods, implant composition, and patient care. Further choices for breast augmentation have been made available to patients by the introduction of alternative methods like fat grafting.

Procedure in general:
A cosmetic operation called breast augmentation surgery, or augmentation mammoplasty, aims to improve the symmetry, size, and form of the breasts. It is one of the most popular cosmetic procedures done globally, and for people looking to feel better about their bodies and boost their confidence, it can be a life-changing operation.
Pre-Surgical Consultation:
Patients usually have a consultation with a plastic surgeon prior to brachioplasty. A physical examination, a review of the patient’s medical history, and a discussion of the patient’s expectations and goals will all be conducted by the surgeon at this consultation to make sure the patient is a good candidate for the procedure.
Deciding on the Type and Size of Implants;
A crucial aspect of breast enhancement surgery involves choosing the type and size of implants. The options typically include saline (saltwater) or silicone gel filled implants, each, with its set of pros and cons. The choice of size is influenced by factors such, as the patient’s desired results, body shape and natural breast tissue.
Having breast augmentation surgery typically takes around one to two hours. Is done while the patient is, under anesthesia. To minimize scarring the surgeon will create an incision either under the armpit around the areola or in the crease of the breast. After forming a pocket either beneath the chest muscle or, behind the breast tissue the implant is inserted into it.
Recovery & Aftercare:
Painkillers and adequate rest can help patients control their swelling, bruising, and discomfort following surgery. The majority of patients can return to their regular activities in a few days to a week, however they should refrain from intense exertion for a few weeks. Additionally, to help with the healing process, patients will be urged to wear supportive bras.
Outcomes:
The immediate aftermath of breast augmentation surgery is evident, but it could take a few weeks for the swelling to completely go down and the final effects become noticeable. The breasts will improve the overall appearance of the chest area by seeming bigger, rounder, and more symmetrical.
Dangers and Complications:
Breast augmentation surgery has dangers, such as bleeding, infection, implant rupture, and changes in nipple sensitivity, just like any other surgical operation. To reduce complications, patients should carefully follow post-operative instructions and discuss these concerns with their physician.
The periareolar method:
Subpectoral: This technique allows for discrete scarring by creating an incision across the lower part of the areola, or the dark area surrounding the nipple. The pectoralis major, a muscle in the chest, is partially covered by the implant, which can seem more natural and lower the chance of capsular contracture, a condition in which the scar tissue surrounding the implant tightens.
Suprapectoral:
In this method, the implant is positioned above the chest muscle, but the lower portion of the areola is still incised. Patients who have sufficient muscular tone and breast tissue may benefit from this therapy.
The Sublime Method:
The subpectoral approach involves making an incision in the inframammary fold, which is the natural fold behind the breast, and positioning the implant beneath the muscle of the chest. This technique helps lessen the chance of rippling or creasing by covering more of the implant.
The implant is positioned above the chest muscle in a suprapectoral technique, which is comparable to the sub pectoral method. Those with limited breast tissue and well-developed chest muscles may find this treatment preferable.
Subpectoral:
To place the implant beneath the chest muscle, a tunnel is built in the axilla, the area just below the armpit. This method prevents breast scarring, however it can be more difficult to put the implants precisely.
Suprapectoral:
An incision is made under the armpit to position the implant above the chest muscle. For patients who would like not have breast scars, this procedure might be appropriate.
Intrapectoral:
Liposuction is used to remove fat from areas of excess fat, including the thighs or abdomen. After processing, the fat is injected into the breast tissue to improve its shape and volume. To get results that look more natural, this procedure can be utilized alone or in conjunction with implants.
Suprapectoral:
Injecting fat above the chest muscle, similar to intrapectoral fat grafting. Patients who want a mild augmentation or who have thin breast tissue may benefit from this treatment.
The periumbilical approach, also referred to as the “belly button” or “TUBA” (transumbilical breast augmentation) strategy, involves creating a tunnel to put the implant after making surgical incision close to the navel. Although there is no scarring on the breast with this method, there are fewer options for implant placement and size.
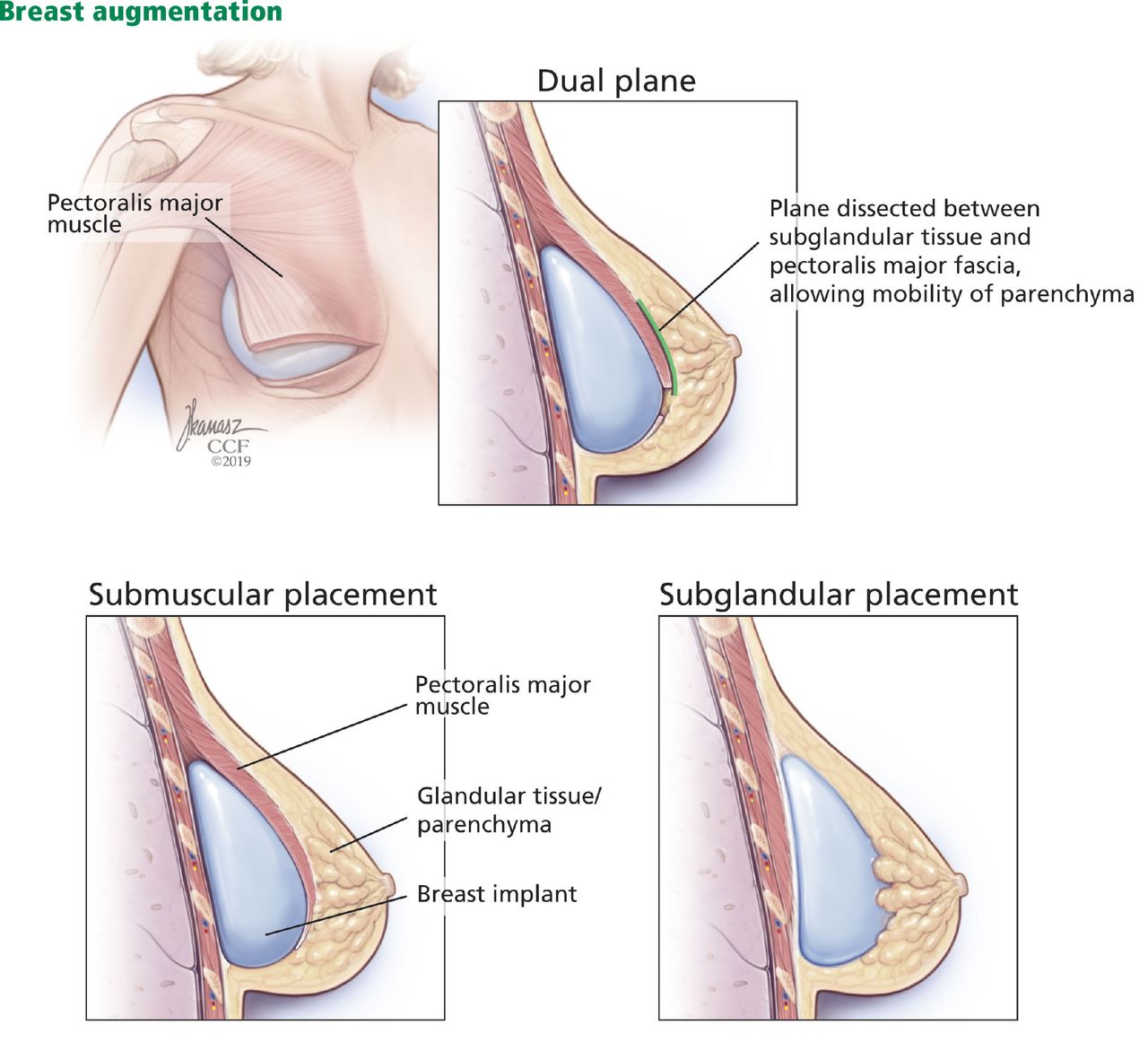
Dual-Plane Technique: This technique allows for a more natural slope and contour to the breast by partially inserting the implant beneath the breast tissue and partially under the chest muscle.
In order to provide a more natural feel and appearance, composite augmentation combines fat grafting with breast implants, especially in patients with limited breast tissue.
Subpectoral Placement:
This method involves the surgeon creating a tunnel for the implantation of implants by making tiny incisions in the transaxillary natural folds of the armpit. Subpectoral, or partially beneath the chest muscle, is where the implant is then placed. With this method, implant insertion may be done precisely and there will be less scarring on the breast.
Suprapectoral implantation:
Suprapectoral implantation involves making transaxillary incisions to situate the implant above the chest muscle. Patients desiring a more natural appearance and possessing sufficient muscle tone and breast tissue may find this method appropriate.
Subpectoral Placement:
To access the breast tissue, the surgeon uses the short scar periareolar approach, which involves making an incision around the lower half of the areola. Through this incision, the implant is then partially positioned under the subpectoral muscle of the chest. This method offers access for accurate implant implantation with the least amount of scarring.
Method of Vertical Incision:
Subpectoral Placement:
The vertical incision approach entails creating a vertical incision that runs from the inframammary fold to the base of the areola. Through this incision, the implant is then partially positioned under the subpectoral muscle of the chest. Precise implant implantation and access to the breast tissue are made possible by this method.
Suprapectoral Placement:
In this technique, a vertical incision is used to insert the implant above the chest muscle. For patients who have sufficient muscular tone and breast tissue, this procedure might be chosen.
Sculpting Methods:
Subpectoral Placement:
In order to produce a more aesthetically pleasing contour, sculpting techniques entail molding the breast tissue and chest muscle. To improve volume and contour, the implant is partially positioned under the subpectoral muscle in the chest. This method yields outcomes that look natural and enables for modification of the implant pocket.
Suprapectoral implantation:
To obtain the desired contour, the implant is positioned above the chest muscle using suprapectoral implantation in conjunction with sculpting procedures. Patients with limited breast tissue and well-developed chest muscles may benefit from this therapy.
The advantages and considerations of each of these techniques vary, thus the surgeon's experience, the anatomy of the patient, and the intended result should all be taken into account while selecting a technique. To choose the best course of action for their unique needs, patients should talk through their options with their surgeon.
Benefits, Comparisons and consideration:
The periareolar method Benefits:
With the subpectoral procedure in particular, this method provides little scarring and accurate implant placement. It also gives you access to change the nipple's position if needed.
Preferences:
Since the chest muscle offers extra coverage for the implant, subpectoral placement is frequently chosen for individuals with thin breast tissue or those who are at risk of capsular contracture. Patients with enough breast tissue and muscular tone may benefit from suprapectoral implantation.
Changes in nipple feeling, obvious scarring, and capsular contracture—the development of scar tissue surrounding the implant that may result in breast firmness or deformity—are possible complications.
Subliminal Method:
Benefits:
This method's direct access makes implant installation and adjustment simpler. Patients with well-developed chest muscles might benefit from it.
Preferences:
Patients who want a more natural appearance or who have less breast tissue may choose subpectoral placement since the muscular coverage can help lower the chance of noticeable wrinkling or rippling. For patients with sufficient breast tissue, suprapectoral implantation might be the preferred option.
Complications:
Visible scarring, implant displacement, and capsular contracture are possible complications.
Transaxillary Method:
Benefits:
Patients who are worried about obvious scars may find this method intriguing as it prevents scarring on the breast. It allows access for the implantation of implants without causing any direct damage to breast tissue.
Preferences:
Patients with thin breast tissue should have subpectoral placement since the muscular coverage can contribute to a more realistic appearance. In patients with sufficient muscular tone and breast tissue, suprapectoral implantation may be good.
Problems with implant adjustment, noticeable scars under the arms, and incorrect placement of the implant are examples of complications.
Grafting Fat:
Benefits:
Fat grafting increases breast volume by using the patient's own fat, giving the breasts a more natural appearance and feel. To obtain the intended result, it can be utilized either alone or in conjunction with implants.
Preferences:
Patients wishing to slightly improve or rectify breast asymmetry, as well as those with excess fat in donor areas such the thighs or belly, can benefit from fat grafting.
Complications:
Uneven fat absorption, which can lead to abnormalities or asymmetry, fat necrosis (the death of fat cells), and cyst formation are examples of complications.
This method, especially for individuals with minor ptosis (sagging), gives the breast a more natural slope and contour. It might, however, be more complicated and need more time to heal.
Composite augmentation:
To create a more natural-looking and feeling breast implant, this treatment combines fat grafting with breast augmentation. Those with little breast tissue will especially benefit from it. On the other hand, it could take longer to recover and necessitates removing fat from donor regions.
Overall, a number of criteria, including as the patient's anatomy, the intended result, and the surgeon's experience, influence the choice of breast augmentation approach. Patients should have a full discussion of their alternatives with their surgeon in order to decide which course of action is appropriate for their unique needs and objectives.
Conclusion:
Finally, it should be noted that breast augmentation surgery has changed dramatically over time, giving patients access to a variety of methods and choices for achieving their desired cosmetic results. Enhancing breast size, shape, and symmetry through breast augmentation remains a safe and successful operation because to developments in surgical techniques, implant materials, and patient safety standards. Under the supervision of a skilled and experienced plastic surgeon, patients can make educated decisions and achieve satisfactory results by studying the history, general procedure, various techniques, and factors related with breast augmentation.
- All Posts

Dr. Daniel Davidson, MD, MBA Introduction: The goal of success for businesses nowadays is to establish a global brand because...

Dr. Daniel Davidson, MD, MBA Introduction: Stem cells have captivated the imagination of scientists and the public alike for their...

Dr. Daniel Davidson, MD, MBA Introduction: Platelet-rich plasma (PRP), fat grafting, and dermal fillers made from natural sources are examples...